Introduction:
Venous thromboembolism (VTE), defined as pulmonary embolism (PE) or deep vein thrombosis (DVT), are often seen with advanced malignancy. Recent studies have demonstrated that the presence of bland IVC or renal vein thrombus at the time of renal cell carcinoma (RCC) surgery is associated with worse outcomes. However, the impact of VTE at time of RCC surgery remains to be understood, particularly among patients without an IVC or renal vein thrombus. We evaluated the morbidity and mortality associated with having concurrent VTE at the time of surgical resection of a renal mass. Costs of care were also compared.
Methods:
We identified 122,342 patients undergoing elective surgical resection for a renal mass from 2013 to 2017 using the Premier Healthcare database, which includes more than 700 non-federal hospitals and translates to over 20% of annual discharges in the United States. The cohort was subdivided based on the presence of VTE at the time of admission for radical nephrectomies (RN) and partial nephrectomies (PN). Patients with renal vein thrombus and/or IVC thrombus were excluded from the analysis. The association of VTE with 90-day non-fatal minor (Clavien 1-2) and major (Clavien 3-4) complication rates, mortality, and direct hospital costs (2019 US dollars) was determined with multivariable logistic regression and quantile regression models, respectively, adjusting for patient, hospital, and surgical characteristics.
Results:
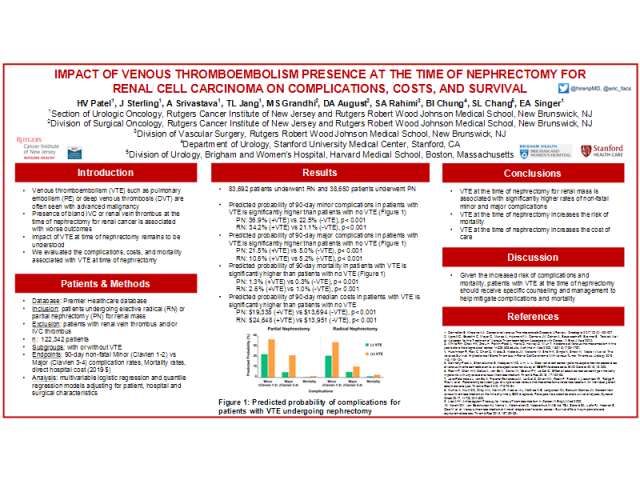
Of the total study population, 83,692 patients underwent RN and 38,650 patients had PN. The predicted probability for a non-fatal minor complication in patients with VTE was significantly higher than patients with no VTE undergoing RN and PN (RN: 34.2% vs 21.1%; PN: 36.9% vs 22.5%; p<0.001). The predicted probability for a non-fatal major complication in patients with VTE was significantly higher than patients with no VTE undergoing RN and PN (RN: 10.6% vs 5.2%; PN: 21.5% vs 5.0%; p<0.001). The predicted probability of mortality in patients with VTE was significantly higher than patients with no VTE undergoing RN and PN (RN: 2.6% vs 1.0%; PN: 1.3% vs 0.3%; p<0.001). The 90-day median costs were greater in patients with VTE compared to no VTE undergoing RN and PN (RN: $24,648 vs $13,951; PN: $19,338 vs $13,694; p <0.001).
Conclusion:
VTE at the time of renal surgery for suspected RCC is associated with significantly higher rates of major complications, increased mortality, and higher overall costs. Taken together, these findings may have important implications for the counseling and management of patients with renal masses and VTE.
Funding: National Cancer Institute (P30CA072720)
Image(s) (click to enlarge):
THE IMPACT OF VENOUS THROMBOEMBOLISM PRESENCE AT THE TIME OF NEPHRECTOMY FOR RENAL CELL CARCINOMA ON COMPLICATIONS, COSTS, AND SURVIVAL
Category
Kidney Cancer > Advanced
Description
Poster #79
-
Presented By: Hiren V. Patel
Authors:
Hiren V. Patel
Joshua Sterling
Arnav Srivastava
Thomas L. Jang
Miral S. Grandhi
David A. August
Saum A. Rahimi
Benjamin I. Chung
Steven L. Chang
Eric A. Singer