Introduction:
Prostate cancer is the most frequently diagnosed solid organ cancer in men in the United States. For low-risk disease, active surveillance (AS) has become the standard of care due to the low rate of prostate cancer mortality and relative morbidity of definitive treatment. For intermediate-risk disease, some patients can have a similar indolent course. While studies indicate AS can be a feasible and safe option for certain patients with intermediate-risk disease, current use of AS for this population remains unclear. Accordingly, we characterized and assessed trends of AS among patients with low- and intermediate-risk prostate cancer.
Methods:
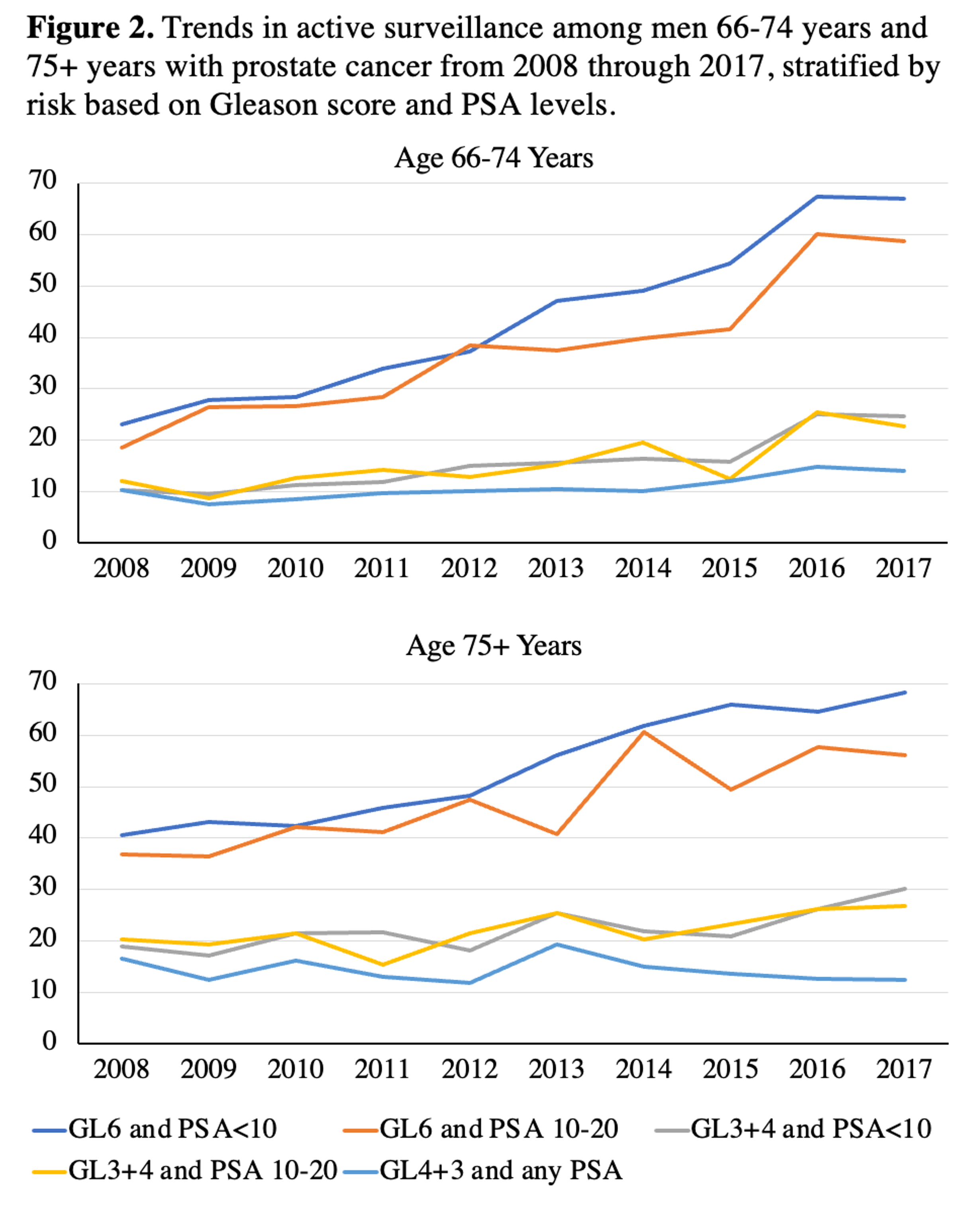
Using linked SEER-Medicare data, we identified men 65 years and older diagnosed with localized low- and intermediate-risk prostate cancer from 2008–2017. We defined low-risk prostate cancer as those with Gleason 3+3 with PSA <10 and intermediate-risk prostate cancer as those with Gleason 3+4 or PSA ≥10. We then subdivided intermediate-risk cancer into specific groups – Gleason 3+3 with PSA 10-20, Gleason 3+4 with PSA<10, Gleason 3+4 with PSA 10-20, and Gleason 4+3 with any PSA – and examined overall trends in use of AS (defined as absence of claims for surgery, radiation, androgen deprivation therapy, or chemotherapy within 12 months of diagnosis) as well as trends sub-stratified by age group (i.e., 65-74 vs. 75+), using the Cochran-Armitage Trend Test.
Results:
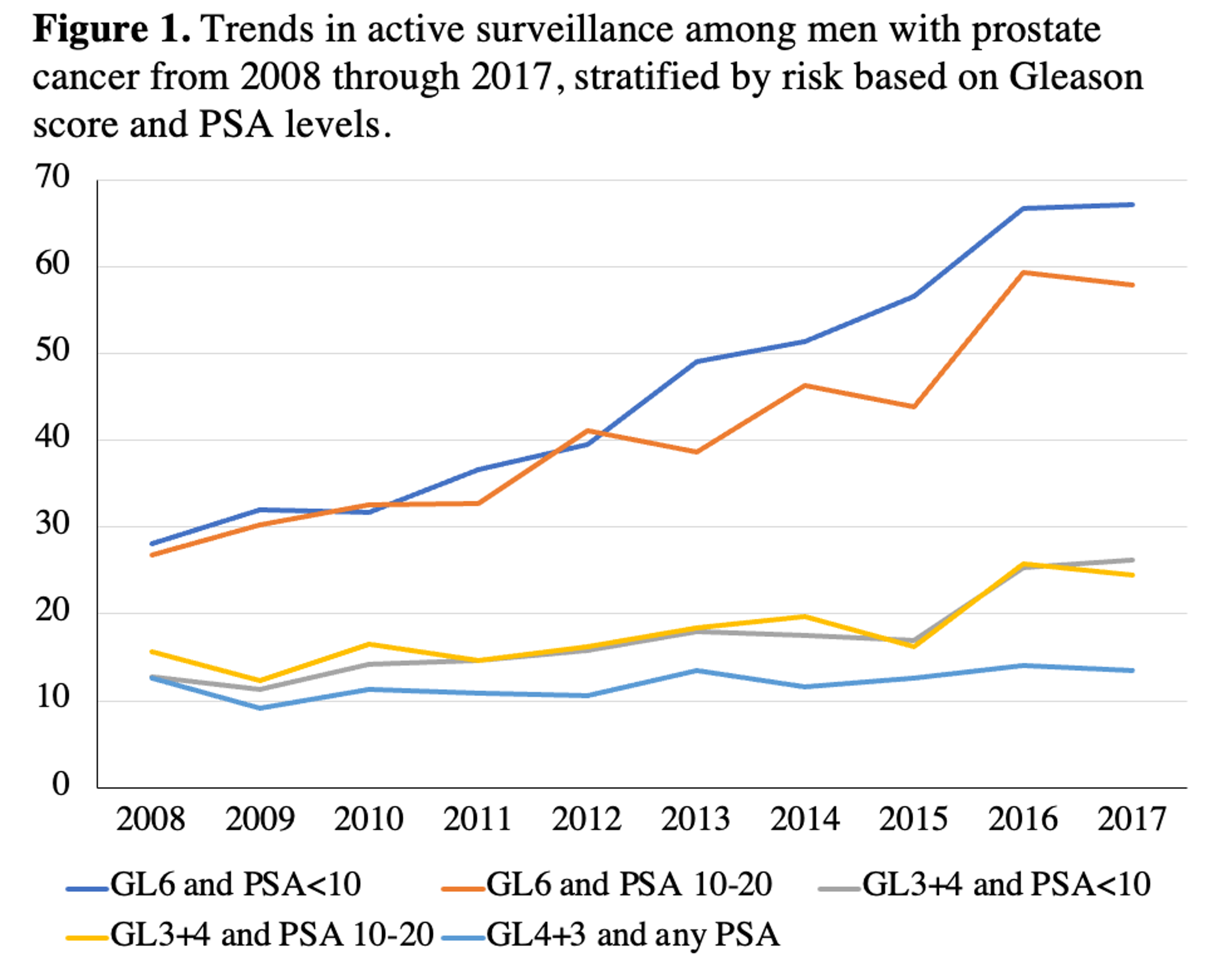
From 2008 to 2017, 27,010 men presented with low-risk and 38,133 men presented with intermediate-risk prostate cancer. Among intermediate-risk patients, 4,457 (11.7%) were categorized Gleason 3+3 with PSA 10-20, 18,413 (48.3%) Gleason 3+4 with PSA<10, 4,088 (10.7%) Gleason 3+4 with PSA 10-20, and 11,175 (29.3%) with Gleason 4+3 with any PSA. Use of AS significantly increased across all groups except for men with Gleason 4+3 (Figure 1 and 2). Specifically rates of AS increased from 28.1 to 67.2% for Gleason 3+3 with PSA<10 (p<0.0001), 26.8 to 57.9% for Gleason 3+3 with PSA 10-20 (p<0.0001), 12.7 to 26.2% for Gleason 3+4 with PSA<10 (p<0.0001), and 15.7 to 24.5% for Gleason 3+4 with PSA 10-20 (p<0.0001). The proportion of men with Gleason 4+3 receiving AS stayed stable.
Conclusion:
Active sruveillance for men with intermediate-risk prostate cancer has increased significantly in recent years. In particular, men with Gleason 3+3 disease and PSA 10-20 appear to be approaching AS levels of their counterparts with low-risk disease, highlighting the importance of Gleason score in treatment selection. Additional research is needed to define other determinants of active surveillance in this patient population.
Funding: The database infrastructure used for this project was funded by the CER Strategic Initiative of UNC’s Clinical &Translational Science Award (UL1TR002489), the UNC School of Medicine, and the UNC Lineberger Comprehensive Cancer Center’s University Cancer Research Fund (UCRF) via the State of North Carolina.
Image(s) (click to enlarge):
Contemporary Trends in Active Surveillance for Men with Low- and Intermediate-Risk Prostate Cancer among Older Men: a SEER-Medicare Analysis
Category
Prostate Cancer > Potentially Localized
Description
Poster #65
Thursday, Dec 2
9:00 a.m. - 10:00 a.m.
Prostate 1
Presented By: Brooke Namboodri Spratte
Authors:
Brooke Namboodri Spratte
Soohyun Hwang, MPH
Ram Sankar Basak, PhD
Ibardo Zambrano, MD
Hung-Jui Tan, MD, MSHPM