Introduction:
Renal medullary carcinoma (RMC) is a renal malignancy that afflicts young persons of African descent with sickle hemoglobinopathies. RMC is aggressive and resistant to therapies used routinely in RCCs. More than 90% will be diagnosed with advanced disease and have a theraputic objective response rate of 29% with a 13 month median survival. Therefore, there's a need to develop new ways to screen, diagnose, and treat RMC in order to raise its survival curve. To meet this need we established a large RMC cohort and assessed known serum tumor markers with RMC disease severity (e.g.metastatic burden) and correlated marker levels to theraputic response. We hypothesized the magnitude of marker CA-125 within a patient’s body correlated to disease severity and can be used as a therapeutic target. We aim to evaluate CA-125 levels, with other tumor markers (CA19.9, CA15.3, CEA, LDH, AFP) and correlate these with disease burden and treatment response.
Methods:
Using a prospective, IRB-approved collection protocol, serum markers were captured from the medical record in patients with primary RMC. All patients were pooled into a de-identified HIPAA compliant password-protected database with restricted access. A database search of all RMC patients that were treated at MD Anderson within the past 10 years was conducted. Those without serum tumor markers available for review were excluded. Inclusion criteria required a diagnosis of RMC to be confirmed with tissue either from biopsy or final nephrectomy specimen. Using routine serum tests, known tumor biomarkers in other malignancies were assessed to determine differences in magnitude for a given patient with metastatic RMC. These tumor markers included CA-125, CEA, AFP, CA19.9, CA15.3 and LDH and trended over time with respect to key clinical events within the cohort including treatment regimens, responses, relapses, and progression of disease.
Results:
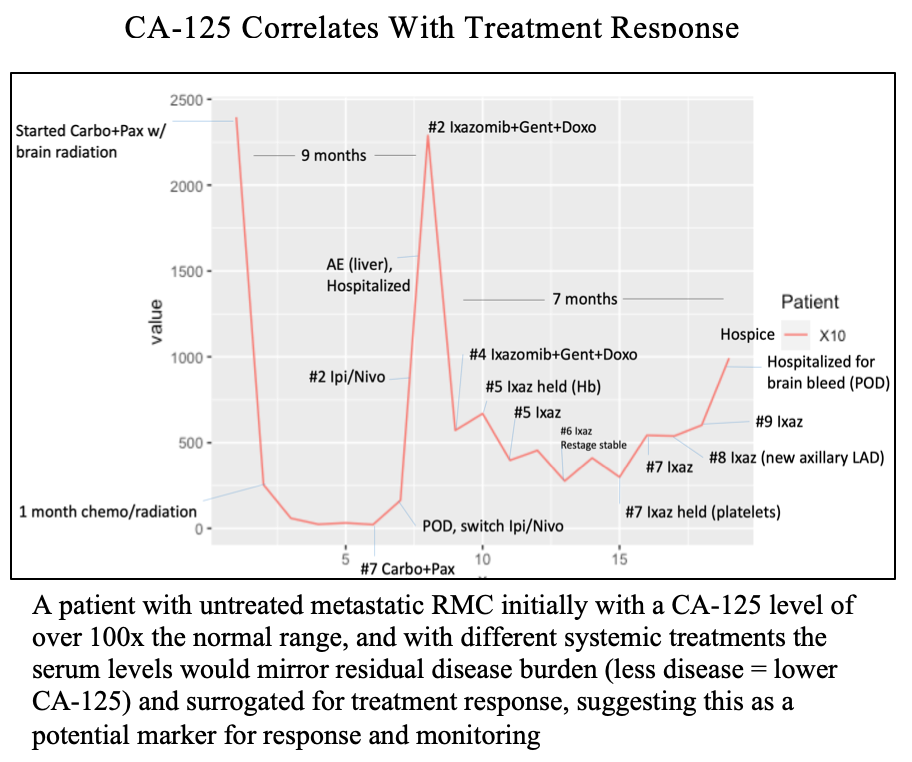
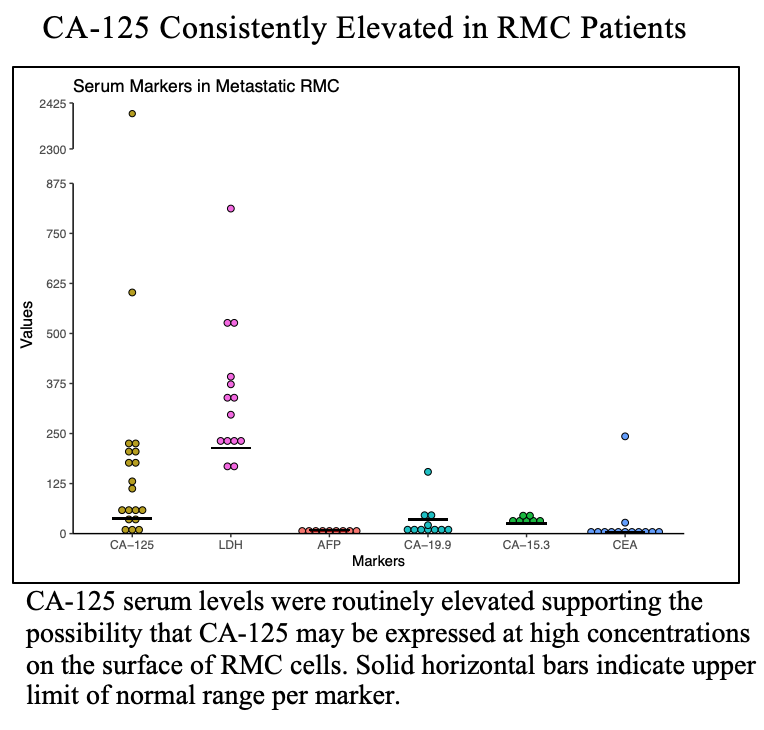
Eighteen patients met inclusion criteria. Median age was 30 years, comprised of 72% male, 94% Black race, with 78% carrying hemoglobinopathy (e.g.sickle-cell trait). Approximately 89% were metastatic at presentation, with an average follow-up of 5.8 months. Higher levels of CA-125 in RMC patients was observed. In metastatic patients, CA-125 was 20-100x above normal, and during treatment convalescence, these values recessed back to lower levels. Similarly, we observed that throughout systemic treatment, responses correlated with CA-125 levels. For instance, positive treatment response resulted in less circulating CA-125 and this could be measured over time (Figure). We observed LDH and CA-125 were consistently elevated above upper-limit normal ranges, unlike markers AFP, CA19.9, CA15.3, and CEA (Figure). Intriguingly, that magnitude of LDH and CA-125 elevation correlated to amount of metastatic burden (brain and liver vs bone only), with CA-125 levels in widely metastatic patients sometimes 200+% higher than upper limit of normal ranges.
Conclusion:
Trending levels of serum biomarkers such as CA-125 in RMC may assist in (1) predicting development or location of metastatic disease, (2) speed the development of biomarkers for treatment response and resistance, (3) correlate to treatment response or efficacy, (4) identify a new therapeutic target. Further work to evaluate the expression of such markers on the cell surface of RMC cells is currently ongoing.
Funding: N/A
Image(s) (click to enlarge):
BIOMARKERS OF DISEASE BURDEN AND TREATMENT RESPONSE IN RENAL MEDULLARY CARCINOMA
Category
Kidney Cancer > Basic
Description
Poster #121
Thursday, December 1
1:00 p.m. - 2:00 p.m.
Presented By: Kyle A. Blum
Authors:
Kyle A. Blum
Pavlos Msaouel